This is the third post in a multi-part series about the American Academy of Pediatrics (AAP) and their policies on children’s gender and sexual health. If you don’t know who I am, check out my Re:Introduction. If you’d like to start at the beginning, here is the first post of the series.
My previous post in this series was a bite-sized book report presenting some feminist ideas about what accountability is and isn’t. To very briefly review, accountability is an approach to repairing harm between people. Accountability involves voluntarily engaging in reflection to understand how a person’s actions have affected other people and voluntarily committing to change and restorative processes to address wrongdoing. To be accountable is to tell a story about the past that honors the perspectives of the people who have been harmed. What’s crucial to accountability is that the story of “what happened” directly acknowledges that harm occurred instead of making excuses or justifications for why someone did what they did.
You may have noticed that it’s been a little while (nearly 3 years!) since my last blog post in this series, a blog post which ended with a promise to understand how the AAP might take accountability for the harm caused by its past positions condoning non-voluntary genital cutting of children on the basis of sex. As part of my long, slow quest to fulfill that promise, I helped write a collaborative autoethnography (under review for a special issue of the Journal of Bodies, Sexualities, and Masculinities), presented original research at GLMA‘s 43rd Annual Conference on LGBTQ+ Health, and spoke about inclusive activism at the 2nd annual Intact Global Conference. This work is intended to fill the gap that has been left in conversations about circumcision: rarely do American physicians consider how the person they are circumcising will feel about forced genital amputation.
In the meantime, two members of the AAP’s 2012 Task Force on Circumcision have made new statements about circumcision that contradict the expired 2012 policy statement (expired without renewal as of 2017). Since this series is all about evaluating the judgments and consequences of AAP experts proffering proclamations promoting paternalism and patriarchy, let’s determine if Dr. Andrew Freedman and Dr. Douglas Diekema have been engaging in accountability that helps those who have been harmed to heal, or if these two men are doing something different, something more like doubling down on denial.
Circumcision is “not really a medical practice”
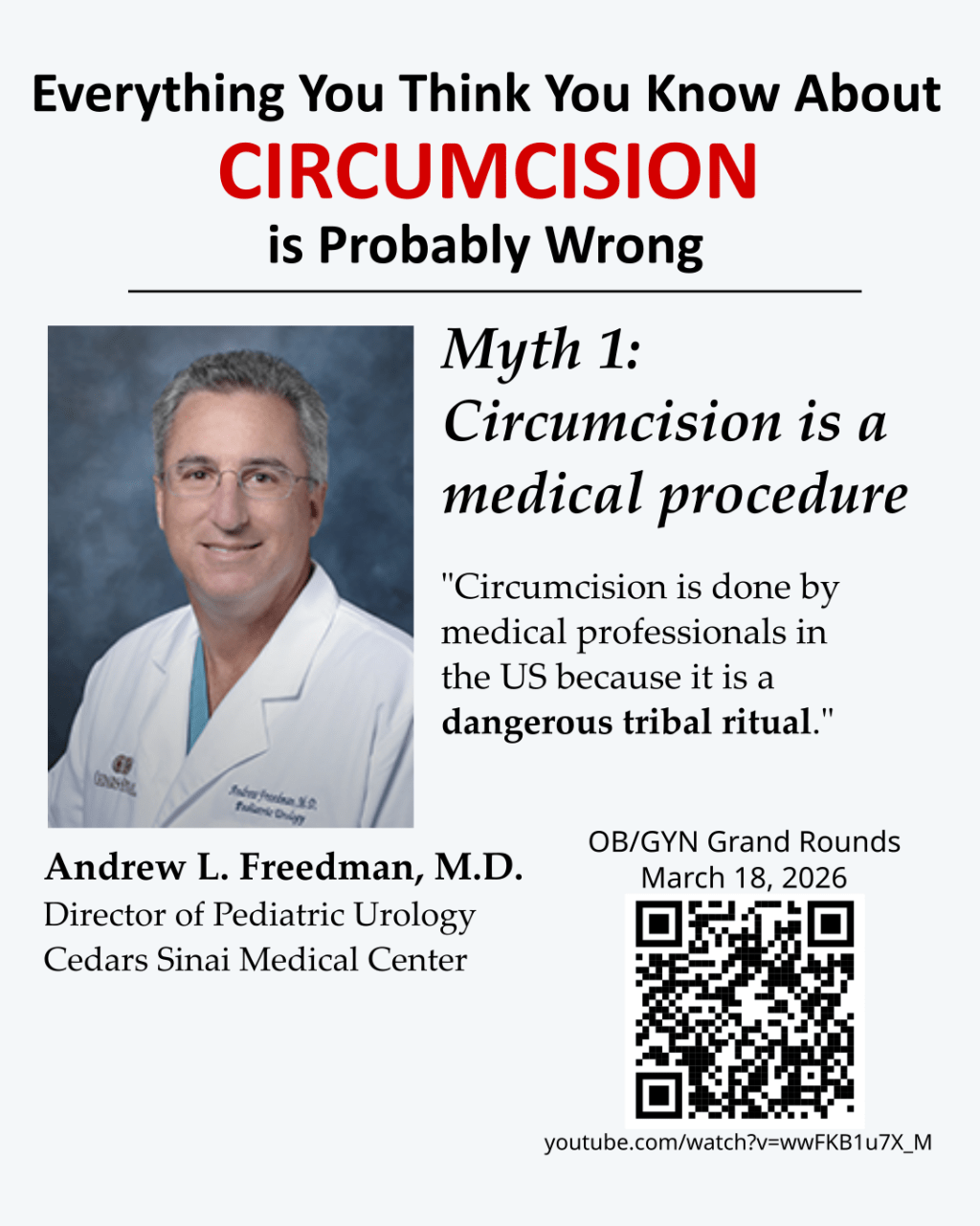
That’s the conclusion of Freedman in the new article by Max Buckler, “As controversies mount, circumcision policies need a rethink” published in the Journal of Medical Ethics in October 2025. Freedman is a puzzling character, even more so since he gave a March 2026 Grand Rounds lecture titled, “Everything You Think You Know About Circumcision is Probably Wrong” which included this list of myths that too many people believe:
Myth 1: Circumcision is a medical procedure
Myth 2: The AAP supports circumcision
Myth 3: Benefits outweigh the risks
Myth 4: Complications are minor and rare
Myth 5: If you have a circumcision, you’ll never have a problem with your penis
Myth 6: Circumcision doesn’t hurt
Myth 7: Circumcision is ethical
Myth 8: Circumcision is only done by OBs
Myth 9: Doctors want to do circumcisions because they are greedy
Myth 10: At Cedars, the process for getting a circumcision works perfectly
That truly is an incredible list of things for Freedman to spell out for physicians and parents. What we are seeing is the reluctant acknowledgement that American believe a lot of false things about circumcision, and interestingly, the fewer false things you believe about circumcision, the less pleased you are with forced circumcision (Earp, Sardi, and Jellison, 2018. False beliefs predict increased circumcision satisfaction in a sample of US American men. Culture, Health & Sexuality).
Whether a genital surgery or amputation was forced on someone or whether it was chosen by them matters a great deal to how a person feels about their genitals being cut. This is why consent is of the utmost importance when it comes to surgery, genitals, and sex. By consent, I don’t mean role-based consent. I don’t mean consent-by-proxy. I mean informed consent given directly by the person whose body will be touched. There is no one more affected by unwanted genital modifications than the person whose body was forcibly modified. Pretending you got consent and approval from the person you’re cutting into when you truly did not is not good enough when it comes to genital amputation.
Using humor to neutralize empathy: circumcision jokes and rape jokes
Tellingly, Freedman does everything but acknowledge that there are many people who feel harmed — emotionally, spiritually, physically — by unwanted circumcision. He never allows himself a moment of empathy for circumcision sufferers, never once acknowledging that circumcision sufferers exist.
I felt like throwing up when, during his grand rounds lecture, he invited his audience to laugh at jokes while displaying images of children’s circumcised genitals that had been badly scarred, damaged, and mutilated by an adult. These images of children’s injured genitals should invite an attitude of extreme sensitivity and reverence for the needless violence that is happening to a vulnerable population, but in the exact moment when we would be called to empathize with the children whose genitals had been so badly abused, Freedman instead invites us to dehumanize those children with mockery. It is truly sickening to witness the moral inversion happen.
Freedman claims that the conversation we should be having about circumcision is the one about ethics. Let’s do it, Dr. Freedman. Let’s have that conversation. But you and I cannot have that conversation until you acknowledge the existence of circumcision sufferers like me. We are real. Our complaints are justified. We want you to stop cutting children without their assent. We want you to treat patients with more respect. A conversation about ethics can only “take place in a context where there is an ability to speak across difference, and that requires the people at the table being minimally understood as real subjects (Hemmings, C. (2022) “But I thought we’d already won that argument!”: “Anti-gender” Mobilizations, Affect, and Temporality).”
Pediatricians must ground their ethics in children’s rights
In his Grand Rounds, Freedman presents a cartoon model of ethics as a way of explaining to the audience how he personally justifies circumcision despite circumcision not being a medical procedure. What Freedman offers is truly unimpressive, and there is no indication he followed the recommendations of his fellow former Task Force member Diekema, who urged people to acknowledge and address the recent bioethical work that explains the unethical nature of circumcision. It is not like Freedman cites some robust body of ethics literature. It may be hard to believe, but the ethical logic behind the last 15 years comes down to little more than this: Freedman believes parents have a right to do what they want to children so long as we think of parents as loving and benevolent. He is a parent’s rights radical, and he uses parent’s rights as a central justification for perpetuating forced genital cutting.
That is not a standard view of medical ethics. For a contrast, let’s look at Cultural Considerations and Child Maltreatment: In Search of Universal Principles by Gauri Kolhatkar, MD, MPHa and Carol Berkowitz, MD, (Pediatr Clin N Am http://dx.doi.org/10.1016/j.pcl.2014.06.005)
“Practitioners must consider the physical and emotional harm done to the child in addition to cultural aspects of parental intent.”
“A culturally respectful approach does not necessitate universal tolerance of all cultural practices. Abney cautions that relativism may predispose to the acceptance of a cultural practice without regard to its negative impact. Acts accepted within certain cultures may still be deemed abusive …
Clinicians can be challenged by the tension between maintaining cultural respect while respecting applicable laws, exemplified in the discourse among United States health care providers surrounding female genital mutilation. Nevertheless, adherence to relevant laws surrounding mandated reporting must be respected if child maltreatment is suspected. Failure to report suspicion of maltreatment by a mandated reporter is a criminal offense in most United States jurisdictions punishable by prison and/or a fine. Conversely, mandated reporters in the United States are provided immunity from criminal and civil liability for reporting.”
As Kolhatkar and Berkowitz point out, female genital cutting is an act that providers are recommended to actively prevent and may in fact be held criminally liable for not preventing female circumcision. Freedman’s parent’s rights radicalism runs right up against that recommendation and the law. If a loving, benevolent mom wants to nick or remove her daughter’s clitoral hood, Freedman claims that the way ethics works in America is that physicians should help circumcise the girl. Freedman is just wrong in how he conceives of the ethics of genital cutting.
In reality, physicians have a fiduciary duty to the child to protect the child’s rights and interests, even when the threat to the child’s interests is coming from the child’s own parents. I believe all children deserve such protection regardless of their sex traits. When it comes to why forced genital cutting is emotionally and spiritually harmful to children, it’s worth remembering that feelings of violation and mutilation do not originate from the clitoris. Every person – every child – is capable of feeling violated by unwanted genital cutting, regardless of sex assigned at birth or the typicality of one’s genitals.
Sometimes we don’t need a complicated ethical frame to cut to the heart of accountability. If Freedman were to sit across the table from me, in a candid conversation where we both agreed to take one another’s feelings seriously, and to treat one another as real people, here is what I would say to Dr. Freedman: “If I were regularly touching other people in such a way that made 5% of them feel raped and violated, and someone told me that this was the real world impact of my actions, I would immediately stop touching any additional people that way simply because it is a moral value of mine that I don’t want other people to feel raped and violated by how I treat them. I would not wait for that number to reach 10% or 15% or some higher threshold value before I stopped. I would stop after hearing from the first person brave enough to share their feelings of violation, shame, and grief about my actions. I would not stoop so low as to pretend that the person I hurt is invisible or irrelevant, nor would I make jokes at their expense. That would be unbelievably cruel to do to someone who feels sexually violated by my hand.”
